The following article was published in the Chicago Sunday Tribune on March 5th, 1961.
Do Salk Shots Really Prevent Polio? Should We Keep Using Salk Inoculations? How Good Are the New Oral Vaccines? Here Are the Facts:
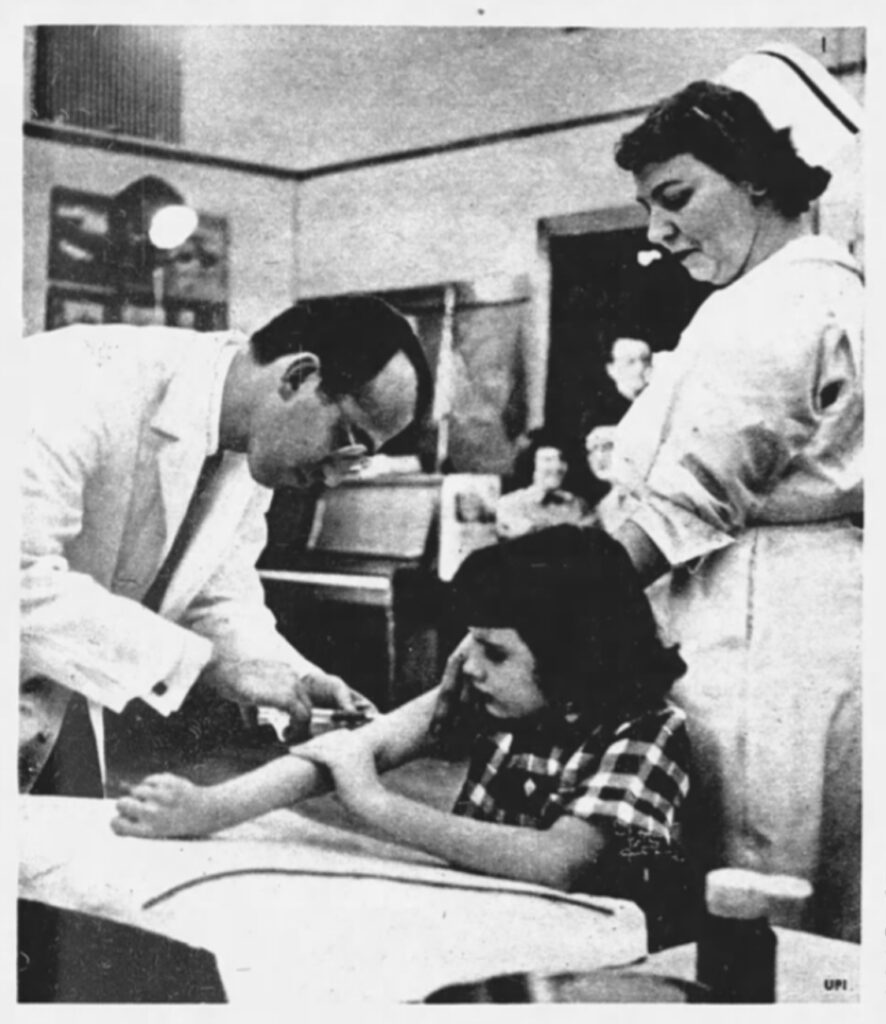
[Image caption] Dr. Jonas E. Salk injects a volunteer with his vaccine in 1954 field trials. Controversial from the first, the Salk vaccine is still a topic hotly debated.
By Joan Beck
BEHIND GLOWING reports of the Salk polio vaccine’s success and even rosier predictions about the new, live, oral Sabin vaccine rages a storm of medical controversy that seldom reaches the ears of parents.
Many serious criticisms have been leveled at the Salk ‘ vaccine. These are now being acknowledged at least indirectly in announcements praising and promoting the new oral vaccines.
Yet all is not yet sweetness and accord among developers of the live, oral vaccines, either. At least three different types have been developed and according to their producers proved safe and effective in tests, chiefly in foreign countries, but also in the United States. One of these new oral vaccines, developed by Dr. Albert Sabin with National Foundation research funds, has been OK’d by the United States public health service for manufacture. But there are problems remaining to be solved in its production and, according to a committee of experts headed by Dr. Roderick Murray of the National Institute of Health, dangers to be considered in its use by the general public (altho it has been given to a reported 77 million Russians and to at least 300,000 Americans. Russian Prof. Mikhail Chumakov, who directed a two year program of inoculation with the Sabin vaccine, says he is convinced polio epidemics have been eliminated in the Soviet Union”). Licensing is not expected until this spring. Quantities of the vaccine are not expected to be available for community-wide use until November.
“Both ‘live (Sabin) and ‘killed’ (Salk) polio-virus vaccines will be needed to combat poliomyelitis in the near future. United States public health officials 8 declared at the A. M. A. clinical meeting,” the Journal of the American Medical association reported in December, 1960. “The new oral poliomyelitis vaccine developed by Dr. Albert Sabin and approved for future use in this country will not be the complete solution as far as can be predicted now, the public health service experts said.”
Evaluating the true effectiveness of the Salk vaccine and the new oral vaccines has been difficult for several reasons. Polio is a relatively rare disease in the United States. Because so few persons get it in its paralyzing form, success of an immunizing agent is hard to determine.
The definition of polio also has changed in the last six or seven years. Several diseases which were often diagnosed as polio are now classified as aseptic meningitis or illnesses caused by one of the Coxsackie or Echo viruses. The number of polio cases in 1961 cannot accurately be compared with those in, say 1952, because the criteria for diagnosis have changed. Even the Salk vaccine itself is not a constant, standard product. Since the first field trials of 1954, the vaccine has been changed several times. The first alterations were aimed at increasing the vaccine’s safety by changing the method of killing the polio virus and by adding an extra filtration step. Newer changes are intended to increase the vaccine’s effectiveness. The success of the Salk vaccine necessarily varies, depending upon which Salk vaccine is being considered.
Ever since the public was first informed about the Salk vaccine in the Francis report of April 12, 1955, the National Foundation has praised its effectiveness and urged parents to have themselves and their children vaccinated. Altho some physicians remained skeptical about the original theories behind the vaccine, about the techniques used in its evaluation, and about its success in combating polio, these objections seldom reached the general public. With the resurgence of paralytic polio in 1958 and 1959, the criticisms increased.
These views were summed up by five experts in a panel discussion on the “Present Status of Polio Vaccines ” presented before the Illinois State Medical society in Chicago, in May, 1960, and published in the August and September issues of the Illinois Medical Journal. To make parents aware of the controversy about the Salk vaccine and the problems involved in developing an effective oral vaccine against polio, here is a report of that discussion:
Moderator of the panel was Herbert Ratner, M. D., director of public health in Oak Park, and associate clinical professor of preventive medicine and public health, Stritch School of Medicine, Chicago.
Dr. Ratner noted the upward trend in polio, particularly in the paralytic form, in the United States during 1958 and 1959. He quoted Dr. Alexander Lang-muir, in charge of polio surveillance for the United States public health service, as saying this resurgence is ” cause for immediate concern.”
“In the fall of 1955, Dr. Langmuir had predicted that by 1957 there would be less than 100 cases of paralytic polio in the United States,” commented Dr. Ratner. “Four years and 300 million doses df Salk vaccine later, we had in 1959 approximately 6,000 cases of paralytic polio, 1,000 of which were in persons who had received three and more shots of Salk vaccine. Salk vaccine hasn’t lived up to expectations.”
Dr. Sabin says the number of cases in 1960 was less than in 1959, but that 23 per cent are now occurring in persons who have had three or more doses of Salk vaccine.
Dr. Ratner next reviewed some basic facts about polio. Paralytic polio occurs in cycles and was in a natural decline when the Salk vaccine was introduced in 1955, he pointed out.
Prior to the introduction of the Salk vaccine, the National Foundation defined an epidemic as 20 or more cases of polio per year, per 100,000 population. Now, an epidemic is defined as 35 cases per year per 100,000. This change has resulted in a statistical but not necessarily a real drop in polio epidemics.
For every case of known paralytic polio, there are about a thousand ” subclinical polio infections,” so mild they pass unnoticed, Dr. Ratner explained. These mild cases account for the high degree of natural immunity in adults. You can have a polio infection in the intestines without having paralytic polio or nonparalytic polio with enough symptoms to be diagnosed.
The theory of the Salk vaccine, made with killed polio virus, is that it will produce enough antibodies circulating in the blood to neutralize poliovirus before it can reach the central nervous system. But ” one of the major disappointments of the killed vaccine ” is that these circulating antibodies do not protect an individual against getting a polio infection in the intestines, nor its breakthru into the circulatory system, said Dr. Ratner. Protection against paralytic polio depends upon the presence of enough circulating antibodies to offset the virus, he explained.

Discussing the “very misleading way” in which the Salk vaccine data has been handled, was Bernard G. Greenberg, Ph. D., head of the department of bio-statistics of the University of North Carolina, school of public health, and former chairman of the committee on evaluation and standards of the American Public Health association.
“There has been a rise during the last two years in the incidence rates of paralytic poliomyelitis in the United States,” stressed Dr. Greenberg. “The rate in 1958 was about 50 per cent higher than that for 1957, and in 1959 about 80 per cent higher than that in 1958. If 1959 is compared with the low year of 1957, the increase is about 170 per cent.
“As a result of this trend in paralytic poliomyelitis, various officials in the public health service, official health agencies, and one large voluntary health organization have been utilizing the press, radio, and television and other media to sound an alarm bell in an heroic effort to persuade more Americans to take advantage of the vaccination procedures available to them,” said Dr. Greenberg.
“Altho such a program might be desirable until live virus vaccines are available to us on more than an experimental basis, the misinformation and unjustified conclusions about the cause of this rise in incidence give concern to those interested in a sound program based on logic and fact rather than personal opinion and prejudice.
“One of the most obvious pieces of misinformation being delivered to the American public is that the 50 per cent rise in paralytic poliomyelitis in 1958 and the real accelerated increase in 1959 have been caused by persons failing to be vaccinated. This represents a certain amount of double talk and an unwillingness to face facts and to evaluate the true effectiveness of the Salk vaccine,” said Dr. Greenberg.
The number of persons over 2 years of age in 1960 who have not been vaccinated cannot be more and must be considerably less than the number who had no vaccination in 1957, Dr. Greenberg pointed out. Then how can it be claimed that it is the large number of unvaccinated persons who are causing the increase in polio, when there were a larger number of unvaccinated individuals in 1957 when the vaccine was given credit for reducing rates of the disease.
“A scientific examination of the data and the manner in which the data was manipulated will reveal that the true effectiveness of the present Salk vaccine is unknown and greatly overrated,” Dr. Greenberg stressed.
Why was there such a tremendous reduction in reported rates of paralytic polio in 1955, 1956, and 1957? Much of this highly publicized decrease was a statistical illusion, said Dr. Greenberg.
Prior to 1954, any physician who reported a case of paralytic poliomyelitis was doing his patient a favor because funds were available to help pay his medical expenses. At that time, most health departments used a definition of paralytic poliomyelitis which specified ” partial or complete paralysis of one or more muscle groups, detected on two examinations at least 24 hours apart.” Laboratory confirmation and the presence of residual paralysis were not required.
In 1955, these criteria were changed. Now, unless there is paralysis lasting at least 60 days after the onset of the disease, it is not diagnosed as paralytic polio.
During this period, too, “Coxsackie virus infections and aseptic meningitis have been distinguished from paralytic poliomyelitis,” explained Dr. Greenberg. “Prior to 1954, large numbers of these cases undoubtedly were mislabeled as paralytic polio.”
Thus, because the definition of the disease was changed and two similar diseases virtually ruled out, the number of cases of polio reported was sure to decrease in the 1955-57 period, vaccine or not. Then, too, physicians are reluctant today to diagnose paralytic poliomyelitis in a vaccinated child without thoro laboratory tests, thus eliminating most of the false positive cases commonly reported in the pre-1954 period.
“As a result of these changes in both diagnosis, and diagnostic methods, the rates of paralytic poliomyelitis plummeted from the early 1950s to a low in 1957,” said Dr. Greenberg. The recent increase in the disease, despite improved diagnostic methods, he believes, is due to a long term, increasing trend in the occurrence of polio.
“Without doubt, the increasing trend has been reduced to some extent by the Salk vaccine,” explained Dr. Greenberg. ” Nevertheless, the Salk vaccine has ‘ limited effectiveness in its ability further to reduce this trend. . . . Any future substantial reduction in this trend will require a more potent vaccine, not simply vaccinating more people.
“Today it may be a serious mistake to be ultra-conservative in accepting the various new live vaccines under the impression that there is no hurry because an almost equivalent immunizer exists in the Salk vaccine. A delay in accepting and promoting better vaccines will be a costly one. There must be immediate pressure applied to determine whether or not the new vaccines are more effective, so that we do not cling, for sentimental or personal reasons, to an older vaccine whose true effectiveness is today unknown.”
The most accurate way we have of determining the effectiveness of vaccine (except by direct exposure to the disease) is to measure the levels of neutralizing antibodies in the blood, explained Herald R. Cox, Sc. D., director of virus research at Lederle Laboratories and president elect of the Society of American Bacteriologists. We do not know, he said, the exact level of antibodies necessary to protect against paralytic polio.
Herman Kleinman, M. D., an epidemiologist from the Minnesota department of health, pointed out that in antibody studies on children who have received three or more doses of Salk vaccine, he has found more than half do not have antibodies to two of the three types of polio strains used in the Salk vaccine. Twenty per cent lack antibodies to a third type.
“This is a very disturbing fact,” said Dr. Kleinman. “If polio antibodies mean anything in respect to protection, then I am forced to conclude that much of the Salk vaccine we have been using is useless.”

[Image caption] Dr. Salk (left) and Dr. Sabin clashes in 1955 hearings about the use of the Salk vaccine.
Dr. Kleinman also commented on the “changing concept of polio” and said physicians were reluctant to diagnose the disease without overwhelming evidence. He called the insistence on a 60 day duration of paralysis in defining paralytic polio ” silly.”
Dr. Cox, who has worked in the virus field since 1929 and was the first person to prove that a killed vaccine could be made, commented on some of the problems of producing a potent, killed-virus vaccine.
“We are now learning, not only in the United States, but in Israel, England, and Denmark, that the killed product does a fairly good job of producing antibodies against Type II poliovirus,” said Dr. Cox. “But Type II represents only about 3 per cent of paralytic cases thruout the world. The killed vaccine does a poor job against Type I, however, which, causes 85 per cent of paralytic cases, and against Type III, which causes about 12 per cent.
“In other words, the killed vaccine is doing its best job against the least important type. It took time to find this out. It was proven in Israel in 1958, when it had its big Type I epidemic. They did not see any difference in protection between the vaccinated and the unvaccinated. Last year in Massachusetts during a Type III outbreak, there were more paralytic cases in the triple vaccinates than in the unvaccinated.”
There have been problems, too, in the production of the killed Salk vaccine. An extra filtration step was added in November, 1955, Dr. Cox said, ” because the amount of formalin used did not inactivate the polio-virus. We found residual live virus for as long as 42 consecutive days of inactivation.”
Dr. Cox went on to assert that the second filtration step was ” picked out of thin air with no experimentation to back it up,” and that the extra filtration cut down on the effectiveness of the vaccine.
Mass vaccination with the Salk product started in April, 1955, and by April 26, there were reports of paralytic polio among vaccinated children, with deaths occurring in Idaho and California. Then came cases of polio among family members of vaccinated children. Live virus was discovered in the supposedly killed vaccine, altho it had been produced by the Salk procedure.
Dr. Ratner cited numerous instances in which live viruses were found in vaccine which was presumably safe, even in Dr. Salk’s own standard vaccines. ” It should be stressed that safety testing was inadequate when Dr. Salk developed the vaccine and when the vaccine was commercially prepared for the field trials of 1954 and for licensing and use in 1955,” said Dr. Ratner. He added that in current vaccine, potency has been sacrificed for safety and that “at present, epidemiologic methods employed by the United States public health service to assure safety of the vaccine are inadequate.”
Should the Salk vaccine continue to be used?
“There is no known way of preventing polio with a licensed product at the present time except thru the use of the Salk vaccine,” answered Dr. Kleinman. “While I am an agnostic about the effectiveness of the Salk vaccine, I still believe it does something in preventing paralysis. So we owe it to the public to recommend its use. On the other hand, if we are going to act not only as public health physicians but as scientists we must continue our investigations into the truth about the Salk vaccine. On the basis of the facts as I know them, we must look for something better.”
Other panel members agreed, pointing out that because all of the facts about the Salk vaccine have not been made public, physicians and public health officials find it difficult to resist the great pressures of public opinion built up thru an unprecedented publicity campaign urging the public to be vaccinated.
“Since nothing else is available, there seems to be no alternative but to push the use of it,” commented Dr. Greenberg. “I don’t think we should do so in ignorance, nor too complacently, believing that as long as we have something partially effective, there is no need to have something better. By being more cautious, we may make a mistake by accepting a better polio vaccine too slowly.”
“When measured against its killed counterpart, a live virus vaccine (using modified virus which stimulate the production of anti-bodies but do not cause the disease) is always a superior vaccine,” asserted Dr. Cox. He said it invariably costs much less. And it gives a higher degree of longer-lasting immunity. Dr. Cox has developed a live vaccine which was tested on thousands of school children and adults last year in Dade county, Fla., and also on thousands of persons in foreign countries.
Another live, oral polio vaccine has been developed by Dr. Hilary Koprowski, of Philadelphia’s Wistar institute and has been tested on approximately 9 million individuals.
Dr. Koprowski has challenged the United States public health service decision last August to grant approval only to the Sabin vaccine. In a letter in the Jan. 14 Journal of the American Medical association, he said, “Altho it is a step forward that the principle of live virus immunization in poliomyelitis has at last been officially accepted, I am taking strong exception to this exclusive indorsement of one set of strains. In my opinion, such an indorsement should evoke a protest from individuals who believe that fair scientific judgment should be the basis for decisions affecting the physical welfare of man.”
Amplifying his letter, Dr. Koprowski said, “It is my belief that government decisions, which are not based on proper evaluation of scientific data, are prompted by either poor choice of scientific advisers or by cryptic reasoning and that such ill-advised decisions could lead to development of an unhealthy climate in which scientists will see their contributions trampled upon by administrative agencies.”
Discussing the development of live, oral vaccines. Dr. Cox explained, “Polio is unique because many more people get the infection than the disease.” The problem in producing a live vaccine is to modify, or tame, the virus so that they will produce a mild infection strong enough to stimulate the formation of antibodies, but not the disease itself. A complicating factor in taming polio virus, is that three separate, tamed strains have to be developed to produce antibodies against the three chief types of polio.
A killed vaccine, such as the Salk, does not immunize an individual against an infection of polio virus in the intestines and, altho it can induce antibodies in the blood, this does not prevent the individual from becoming a carrier and spreading polio-virus, explained Dr. Cox.
Individuals receiving the live, modified, oral vaccines also eliminate poliovirus from their bodies for several days or several weeks after vaccination, but these are the tame, modified strains. Family contacts and even other individuals in the neighborhood can also acquire an immunity from these tame virus, altho they have never received the vaccine themselves.
However, some experts still fear that one of these strains may revert to its virulent type as it is passed from one individual to another, according to a report by Dr. Roderick Murray’s committee, quoted in the Oct. 15, 1960, issue of ” Modern Medicine.” One solution, the committee suggested, might be to give the oral vaccine to entire communities in a brief time. This is a problem which must be solved before the Sabin vaccine is licensed.
Dr. Cox stated that using a live vaccine is the only way to eliminate wild, virulent polio strains in nature. Immunization with live vaccine probably would not protect a person for life, he added, but it would be cheap enough so you could afford it once a year.
Dr. Ratner compared Dr. Cox’s vaccination figures with the 1954 field trials of the Salk vaccine. ” The Cox live poliovirus has now been used by many investigators in over 2.5 million people, the other two live virus vaccines under study have been used in additional millions,” he said. ” Safety has been paramount in the minds of these investigators.”
“On the other hand, Salk vaccine was used in only 400,000 persons in a single field trial which assumed safety and was primarily designed to determine effectiveness.
“An objective and fearless evaluation of the Salk vaccine is needed, for this is the necessary ingredient of an intelligent decision as to when the live virus vaccine should be licensed,” Dr. Ratner continued. ” Obviously, if the Salk vaccine is safe and highly effective, the United States public health service can take its time about licensing the live virus vaccine.
“If, on the other hand, polio and polio epidemics remain with us and children become paralyzed despite three, four, five, and six inoculations of Salk vaccine and vaccinees die, we cannot take our time.”
What should parents do?
Take the advice of their pediatrician or family doctor and not be stampeded by TV commercials or overly-enthusiastic claims for vaccines. It is the individual physician who must decide which vaccine is safe and effective in what circumstances. But physicians must have, honest, impartial, fully scientific information available to make this decision.
Currently, most physicians are still giving Salk vaccine shots. A few doctors do not. Some give them only if patients insist.
Once a live, oral vaccine is fully approved, it will be more effective than the killed Salk vaccine. Because of the doubt about the potency and effectiveness of the Salk vaccine in the past, a full course of the new vaccine will undoubtedly be recommended for everyone, regardless of how many Salk shots each individual has had.
Page 1: https://chicagotribune.newspapers.com/clip/21220730/the-truth-about-the-polio-vaccines/
Page 2: https://chicagotribune.newspapers.com/clip/31494557/the-truth-about-polio-vaccines-pg-2/
Page 3: https://chicagotribune.newspapers.com/clip/31494621/the-truth-about-polio-vaccines-pg-3/
Images of entire article (legible), documented here: https://vaccine.guide/misconduct/data-manipulation/the-truth-about-the-polio-vaccines/