While the mainstream media networks continually claim that the unvaccinated are the cause of the new variants of the SARS-CoV-2 virus / COVID-19, the reality is that vaccines are known to exert additional pressure on viruses to mutate.
The research on this subject describes how “imperfect” vaccines increase pressure on viruses to mutate and become more virulent. “Perfect” vaccines are said to prevent infection and therefore transmission, while “imperfect” ones are known to be “leaky” and do not prevent infection or transmission.
COVID-19 vaccines have definitively been found to be “leaky” and “imperfect”. While the CDC claims they may reduce infection or transmission, they do not prevent infection or transmission.
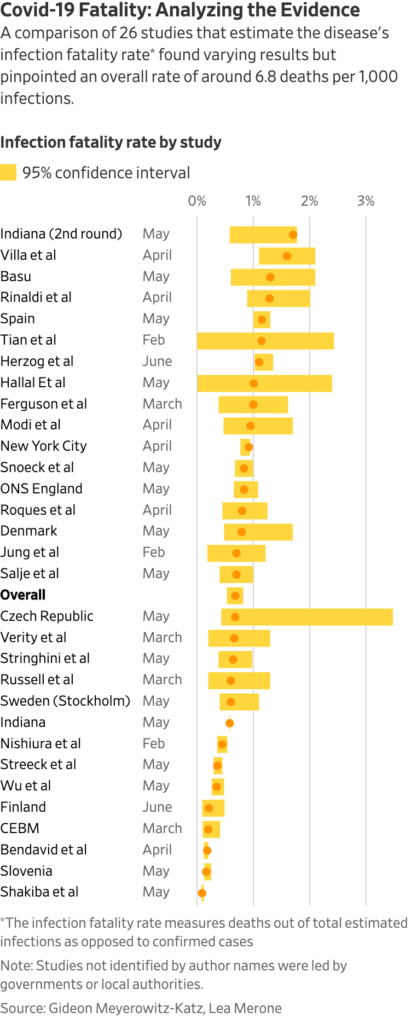
For example, a study of Pfizer’s COVID-19 vaccine determined that protection from infection drops to 20% 5 months after the second dose. With the Delta variant, it was found that the lungs of fully vaccinated individuals carry the same viral load as an unvaccinated person.
While death and complications from infection occur with every virus, in general, most widespread temporary viral infections are benign or even beneficial for the vast majority of relatively healthy or well-nourished individuals. Despite the fear they are associated with, the nature or programming of a virus is to challenge the human body to adapt and improve long term health (and the overall health of the population).
For example, many studies have found that the more febrile (fever-producing) viral infections an individual has during childhood or adulthood, the lower their risk of developing cancers later in life.
On a population and individual level, viruses play an important role. Therefore, when vaccines – such as COVID-19 vaccines – are used in the attempt to thwart a virus, replacing natural infection with an incomplete and leaky defense system, the innate programming of a virus allows it to adapt to fill these gaps. This encourages mutation and the development of new variants.
Researchers from Michigan State University recently confirmed this finding:
“By tracking the evolutionary trajectories of vaccine-resistant mutations in more than 2.2 million SARS-CoV-2 genomes, we reveal that the occurrence and frequency of vaccine-resistant mutations correlate strongly with the vaccination rates in Europe and America.”
When will the vaccine apologists admit that COVID-19 vaccines and Operation “Warp Speed” have been a failure?
Is vaccine failure a new problem?
When it comes to failing to prevent infection or transmission, COVID-19 vaccines are not unique. In fact, nearly every vaccine that has been manufactured and widely administered, could be considered “imperfect”.
While the CDC claims that most traditional vaccines provide longer lasting protection than COVID-19 vaccines, any vaccination that does not result in robust lifetime immunity leaves you with weakening defenses and increased vulnerability to infection over time, especially when antibodies fall to below protective levels. (Of course this is based on the idea that the presence of antibodies is sufficient for immunity, which is not the case.)
Most vaccines that are currently on the CDC schedule are considered to provide a limited duration of protection only, not lifetime immunity. One reason is due to waning antibody levels, however a significant percentage of individuals experience primary or secondary vaccine failure.
Primary vaccine failure is known as an individual not developing antibodies after being vaccinated. Secondary vaccine failure is when an individual who does develop a “protective level” of antibodies becomes infected with the wild-type virus anyway.
For example, research on measles outbreaks have found that not only does primary and secondary vaccination failure occur for the MMR vaccine, but that outbreaks can occur in near-fully vaccinated populations, and the absence of naturally acquired immunity in populations with high vaccine uptake, will eventually lead to a more susceptible population than before the measles vaccination campaign began, as protection diminishes over time.
While the CDC, the mainstream media, the White House, etc. all make very confident claims regarding the effectiveness of vaccines, there’s a massive amount of research and information that is being ignored, sidelined, and censored.
“We simply don’t know what the rules are to inducing long-lasting immunity,” says [Dr. Stanley] Plotkin, who began to research vaccines in 1957. “For years, we were making vaccines without a really deep knowledge of immunology. Everything of course depends on immunologic memory, and we have not systematically measured it.”
– Science, April 2019
Natural infection
On the other side, those who develop natural immunity to wild-type viruses are typically protected for life (e.g. measles, mumps).
While SARS-CoV-2 has been considered a “novel virus”, a label which helped fuel much public fear, those who acquired natural immunity to SARS (SARS-CoV-1) back in 2002-2003 (18 years prior), have been found to have protection from COVID.
In addition, those who acquired natural immunity from SARS-CoV-2 in 2020 have been found to be protected from subsequent variants of the virus (Delta, Omicron, etc.).
As Dr. Stanley Plotkin himself stated, even those who have been engineering vaccines for decades do not have a solid understanding of how the immune system naturally develops immunological memory, let alone how to trigger or successfully mimic this process via vaccination.
The reality is that when a human being contracts a wild virus and acquires immunological memory, they are no longer susceptible to re-infection with the virus nor potential variants, and therefore aren’t actively transmitting it to others. The individual becomes what amounts to a dead-end for the virus. And when a population becomes naturally immune, that is when herd immunity extinguishes transmission completely.
Again, vaccination is almost always imperfect (even according to those who promote vaccines) and therefore unable to provide a lifetime of robust, immunological memory.
Ultimately, the claim that the unvaccinated are the driving force for viral mutation, the creation of new variants, and prolonging this “pandemic” is simply not logical or scientifically sound.
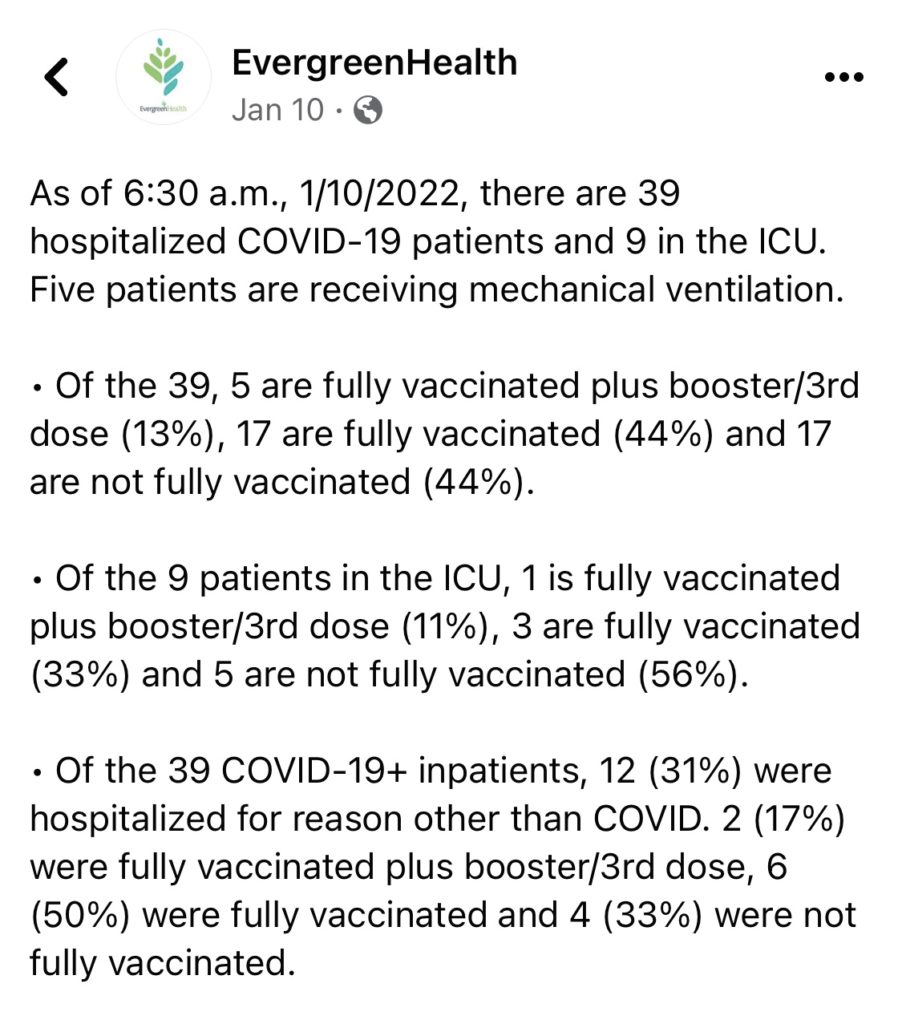
SIDE NOTE: The only other claim the CDC continues to make regarding the “effectiveness” of COVID-19 vaccines is that being fully vaccinated may reduce hospitalization and death from COVID-19.
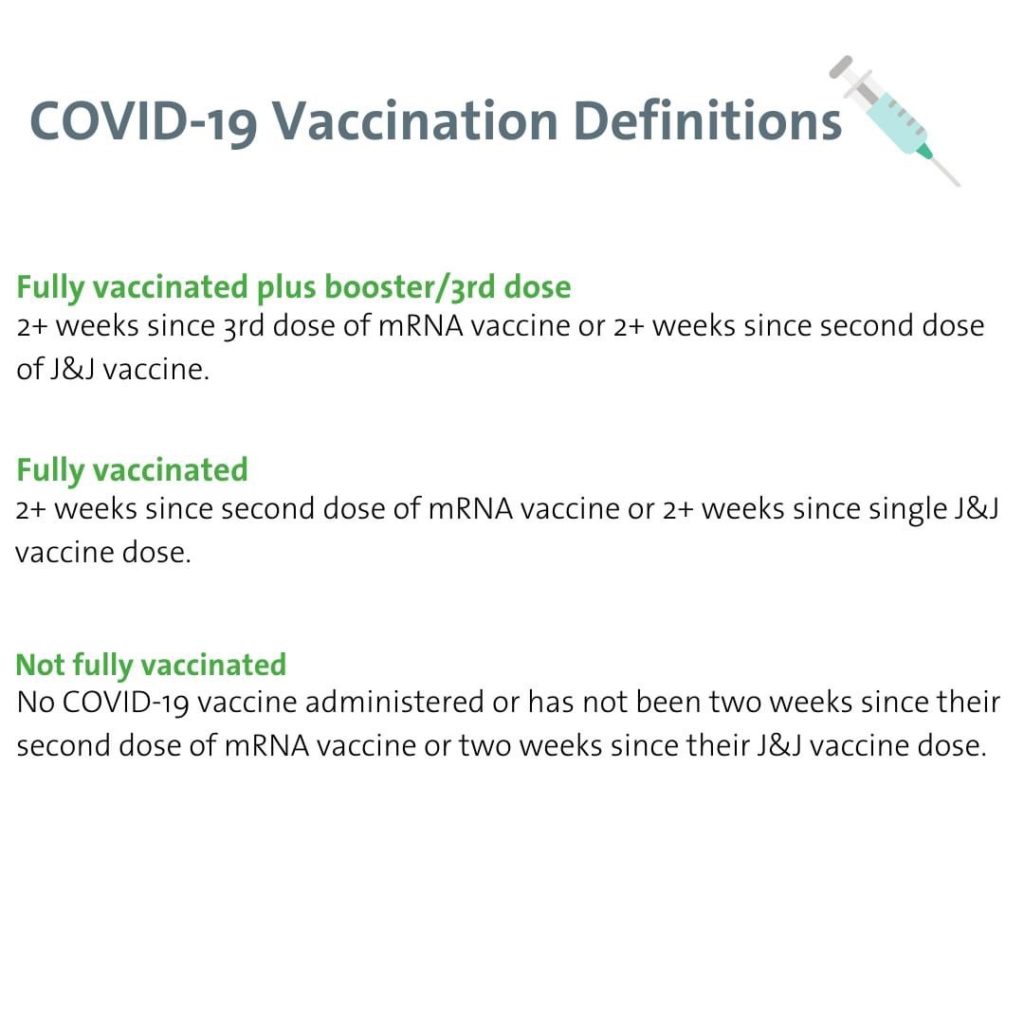
Of course this is based on the following CDC definition of “fully vaccinated”:
Therefore, if you are 13 days past your second dose of the vaccine, you are not considered “fully vaccinated”. Again, every individual who received two doses of the vaccine but is not yet 14 days past their second dose, is tallied under the column of data labeled “not fully vaccinated”:
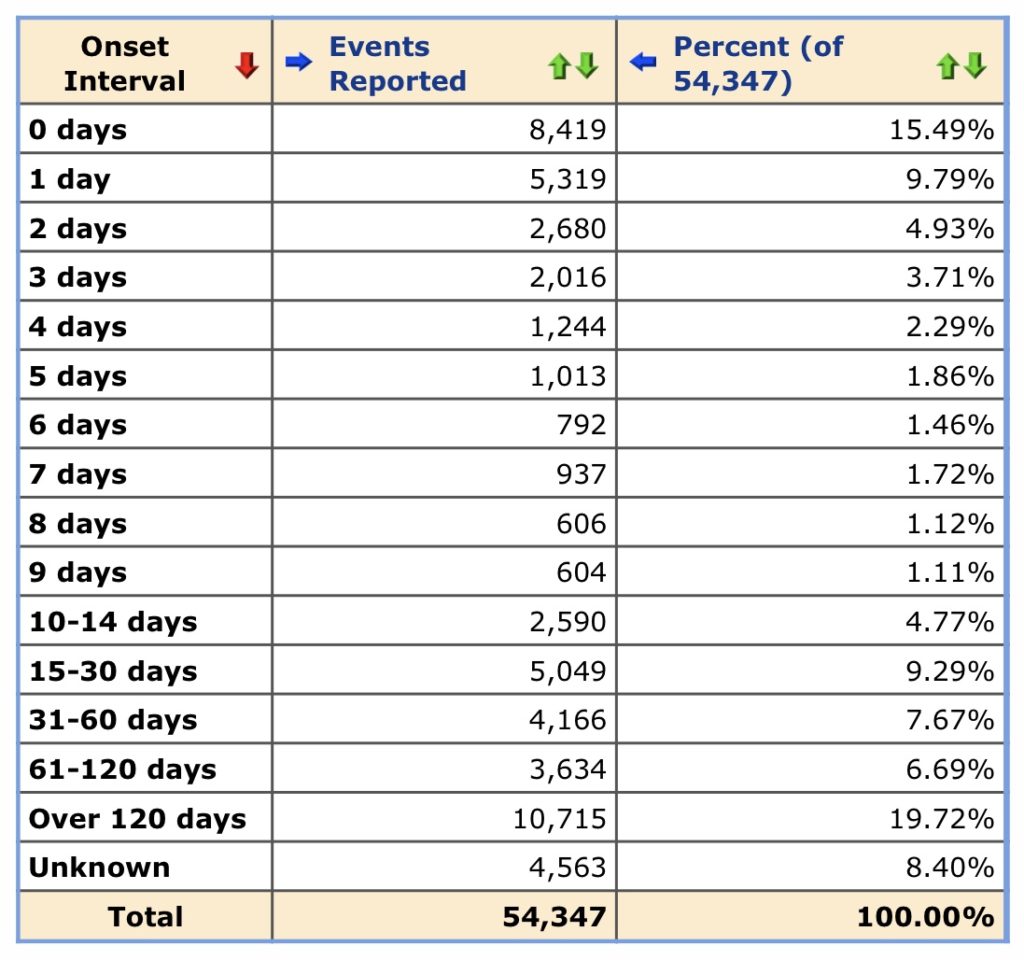
This is how they continue to claim that being fully vaccinated reduces the risk of hospitalization and death. Nearly 50 percent (48.25%) of reported vaccine adverse events post second-dose leading to hospitalization or death, occur within the first two weeks. And we know that adverse events are greatly underreported in general.
SOURCES:
“A peer-reviewed study of 162 Delta-infected index cases and their 231 household contacts—who were tracked and tested every day for up to 20 days, regardless of symptoms—found that once infected, the vaccinated were just as likely to transmit COVID to people in their own households as the unvaccinated: about a quarter of both did so. They also found that the asymptomatic infection rate among vaccinated and unvaccinated participants was similar: around 30 percent.”
The Risk of Vaccinated COVID Transmission Is Not Low https://www.scientificamerican.com/article/the-risk-of-vaccinated-covid-transmission-is-not-low/?amp=true
“Vaccinated people can still become infected and have the potential to spread the virus to others…”
“For the Delta variant, early data indicate vaccinated and unvaccinated persons infected with Delta have similar levels of viral RNA and culturable virus detected…”
COVID-19 Vaccines and Vaccination https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/fully-vaccinated-people.html Updated Sept 2021.
“A new study from the University of California, Davis, Genome Center, UC San Francisco and the Chan Zuckerberg Biohub shows no significant difference in viral load between vaccinated and unvaccinated people who tested positive for the delta variant of SARS-CoV-2.”
Viral Loads Similar Between Vaccinated and Unvaccinated People https://www.ucdavis.edu/health/covid-19/news/viral-loads-similar-between-vaccinated-and-unvaccinated-people Oct 2021.
An emerging SARS-CoV-2 mutant evading cellular immunity and increasing viral infectivity https://www.biorxiv.org/content/10.1101/2021.04.02.438288v1
“Here, we demonstrate that vaccine-breakthrough or antibody-resistant mutations provide a new mechanism of viral evolution . . . By tracking the evolutionary trajectories of vaccine-resistant mutations in more than 2.2 million SARS-CoV-2 genomes, we reveal that the occurrence and frequency of vaccine-resistant mutations correlate strongly with the vaccination rates in Europe and America. We anticipate that as a complementary transmission pathway, vaccine-breakthrough or antibody-resistant mutations, like those in Omicron, will become a dominating mechanism of SARS-CoV-2 evolution when most of the world’s population is either vaccinated or infected.”
Mechanisms of SARS-CoV-2 Evolution Revealing Vaccine-Resistant Mutations in Europe and America https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC8672435/ (2021)
Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00648-4/fulltext (2021)
“Results: The data reviewed in this article support earlier observations on the topic, i.e. that the occurrence of fever in childhood or adulthood may protect against the later onset of malignant disease and that spontaneous remissions are often preceded by feverish infections.
Conclusion: Pyrogenic substances and the more recent use of whole-body hyperthermia to mimic the physiologic response to fever have successfully been administered in palliative and curative treatment protocols for metastatic cancer.”
Fever, Cancer Incidence and Spontaneous Remissions https://pubmed.ncbi.nlm.nih.gov/11549887/ (2001)
“Primary [vaccine] failure arises when a vaccinated individual does not develop a humoral response. Secondary failure occurs when an individual develops specific IgG antibodies after vaccination but exhibits no protection against subsequent infection with a wild-type virus. Secondary failure is characterized by the absence of a primary immune response, i.e., IgM, with the presence of high-avidity virus-specific IgG antibodies at the time of symptomatic acute infection.”
Measles, the need for a paradigm shift https://link.springer.com/article/10.1007/s10654-019-00569-4 (2019)
Mild Measles and Secondary Vaccine Failure During a Sustained Outbreak in a Highly Vaccinated Population. https://pubmed.ncbi.nlm.nih.gov/2278542/ (1990)
“Waning levels of measles antibodies with increasing time post-vaccination suggests that measles susceptibility is potentially increasing in Korea. This trend may be related to limitations of vaccine-induced immunity in the absence of natural boosting by the wild virus, compared to naturally acquired immunity triggered by measles infection. This study provides an important view into the current measles herd immunity in Korea.”
An increasing, potentially measles-susceptible population over time after vaccination in Korea https://www.sciencedirect.com/science/article/pii/S0264410X17308551 (2017)
“a growing body of evidence [suggests] that the protective immune responses triggered by flu vaccines wane in a matter of weeks…”
“It’s not just flu. Recent studies show vaccines for mumps, pertussis, meningococcal disease, and yellow fever also lose their effectiveness faster than official immunization recommendations suggest.”
“…vaccines are approved and come to market years before it’s clear how long protection lasts. Later, fading protection can go unnoticed…”
“‘We simply don’t know what the rules are to inducing long-lasting immunity,’ says Plotkin, who began to research vaccines in 1957. ‘For years, we were making vaccines without a really deep knowledge of immunology. Everything of course depends on immunologic memory, and we have not systematically measured it.’”
How long do vaccines last? https://www.science.org/content/article/how-long-do-vaccines-last-surprising-answers-may-help-protect-people-longer (2019)
“…multiple epidemiological and clinical studies, including studies during the recent period of predominantly delta (B.1.617.2) variant transmission, found that the risk of repeat SARS-CoV-2 infection decreased by 80.5–100% among those who had had COVID-19 previously. The reported studies were large and conducted throughout the world.
Another laboratory-based study that analysed the test results of 9,119 people with previous COVID-19 from Dec 1, 2019, to Nov 13, 2020, found that only 0.7% became reinfected.
In a study conducted at the Cleveland Clinic in Cleveland, OH, USA, those who had not previously been infected had a COVID-19 incidence rate of 4.3 per 100 people, whereas those who had previously been infected had a COVID-19 incidence rate of 0 per 100 people.
Furthermore, a study conducted in Austria found that the frequency of hospitalisation due to a repeated infection was five per 14,840 (0.03%) people and the frequency of death due to a repeated infection was one per 14,840 (0.01%) people.”
“…studies show that protection from reinfection is strong and persists for more than 10 months of follow-up…”
“Researchers have also found that people who recovered from SARS-CoV infection in 2002–03 continue to have memory T cells that are reactive to SARS-CoV proteins 17 years after that outbreak.”
Protective immunity after recovery from SARS-CoV-2 infection https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00676-9/fulltext (2021)
“After the first Pfizer dose, protection against infection was “negligible” for the first 2 weeks but jumped to about 37% in the third week. Protection then reached a peak of about 78% in the first month after the second dose. Efficacy fell gradually after that, with the decline speeding up after the fourth month. For some people who got the vaccine, protection dropped as low as 20% between 5 and 7 months after the second dose.”
Pfizer’s Vaccine Protection May Wane After 2 Months https://www.webmd.com/vaccines/covid-19-vaccine/news/20211008/pfizer-vaccine-protection-may-wane-after-2-months (2021)
“Here we show experimentally that immunization of chickens against Marek’s disease virus enhances the fitness of more virulent strains, making it possible for hyperpathogenic strains to transmit. Immunity elicited by direct vaccination or by maternal vaccination prolongs host survival but does not prevent infection, viral replication or transmission, thus extending the infectious periods of strains otherwise too lethal to persist. Our data show that anti-disease vaccines that do not prevent transmission can create conditions that promote the emergence of pathogen strains that cause more severe disease in unvaccinated hosts.”
“…vaccines that reduce disease but do not prevent infection, replication, and transmission (so-called “imperfect” vaccines) could allow more virulent strains to circulate. Natural selection will even favour their circulation if virulent strains have a higher transmission in the absence of host death or are better able to overcome host immunity. Thus, life-saving vaccines have the potential to increase mean disease virulence of a pathogen population (as assayed in unvaccinated hosts) [2–4].”
“If the vaccine is sterilizing, so that transmission is stopped, no evolution can occur. But if it is non-sterilizing, so that naturally acquired pathogens can transmit from immunized individuals (what we hereafter call a “leaky” vaccine), virulent strains will be able to circulate in situations in which natural selection would have once removed them [2].”
“Note that the possibility of vaccine-driven virulence evolution is conceptually distinct from vaccine-driven epitope evolution (antigenic escape), in which variants of target antigens evolve because they enable pathogens that are otherwise less fit to evade vaccine-induced immunity. The evolution of escape variants has been frequently observed [4,10].”
“…anti-disease vaccines (those reducing in-host replication or pathogenicity) have the potential to generate evolution harmful to human and animal well-being; infection- or transmission-blocking vaccines do not [2–9].”
“Until the 1950s, strains of MDV circulating on poultry farms caused a mildly paralytic disease, with lesions largely restricted to peripheral nervous tissue. Death was relatively rare. Today, hyperpathogenic strains are present worldwide. These strains induce lymphomas in a wide range of organs and mortality rates of up to 100% in unvaccinated birds.”
“…by enhancing host survival but not preventing viral shedding, MDV vaccination of hens or offspring greatly prolongs the infectious periods of hyperpathogenic strains, and hence the amount of virus they shed into the environment.”
“By keeping infected birds alive, vaccination substantially enhances the transmission success and hence spread of virus strains too lethal to persist in unvaccinated populations, which would therefore have been removed by natural selection in the pre-vaccine era.”
“Vaccine failure in the face of virulent pathogens has been documented for at least two viruses other than MDV: feline calicivirus [43] and infectious bursal disease virus in poultry [44]. Both cases are also associated with long-term use of leaky anti-disease vaccines.”
Imperfect Vaccination Can Enhance the Transmission of Highly Virulent Pathogens https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.1002198 (2015)
“Vaccines rarely provide full protection from disease. Nevertheless, partially effective (imperfect) vaccines may be used to protect both individuals and whole populations. We studied the potential impact of different types of imperfect vaccines on the evolution of pathogen virulence (induced host mortality) and the consequences for public health.”
“Previous studies on the evolution of vaccine resistance have focused on the spread of `escape’ mutants that display epitopes different to those in the vaccine, thereby escaping immune recognition – this has already happened for polio and hepatitis B.”
“…as the efficacy of anti-growth-rate and anti-toxin vaccines increases, there is a marked increase in virulence.”
“Because these vaccines do not reduce transmission rate, increased vaccination coverage can increase pathogen prevalence above pre-vaccination levels.”
“Marked increases in virulence of some viral diseases have already followed widespread use of anti-growth-rate vaccines in the chicken industry. When human populations become uncontrolled experimental systems, we recommend that at the very least, intrinsic virulence of the pathogen population (or more realistically, putative virulence determinants such as in vitro multiplication rates) be closely monitored.”
Imperfect vaccines and the evolution of pathogen virulence https://www.nature.com/articles/414751a (2001)
“…the role of vaccination with attenuated viruses on the evolution of wild type strains is not often considered. Antigenic escape because of strong selection by vaccines, emergence of new strains through recombination, and increased virulence to expedite transmission of new genotypes in vaccinated populations are of potential concern.”
“Inactivated vaccines were first made commercially available to the poultry industry in 1946, but because they provided incomplete protection against ND [6], they were replaced with live lentogenic NDV vaccines. Although these vaccines reduce disease, they do not always prevent infection and birds can shed both vaccine and challenge strains of the virus [7,8,9].”
“In this report, we provided evidence that viruses isolated from wild and domestic birds have recombined with vaccine strains, because vaccinated birds are protected from disease but not infection with other strains of aPMV-1. Despite the use of vaccines since the 1950s, the population size of the strain from which the most widely used vaccine was derived has steadily increased. In contrast, other contemporary geno- types, which emerged in the 1960s, experienced a decline in population size in 1998…”
“RNA viruses typically have a high mutation rate due to low fidelity and processivity of their polymerase [25], which coupled with a high replication rate and short generation time [26] lead to high evolutionary rates. In addition, evidence is accumulating that recombination is an important process driving genotype diversity for many RNA viruses [27,28,29].”
“In this study, we explored how vaccination strategies in poultry farming have shaped the evolution of this important avian virus using complete genome sequences available in GenBank.”
“Suboptimal vaccination strategies could also lead to birds becoming infected with both a vaccine strain and circulating genotype, which can alter viral virulence [16].”
“This raises concerns that modified live virus vaccines, although efficacious, may facilitate emergences of new strains with unpredictable phenotypes through recombination with circulating viruses.”
The effect of vaccination on the evolution and population dynamics of avian paramyxovirus-1 https://pubmed.ncbi.nlm.nih.gov/20421950/ (2010)
“Coronaviruses (CoVs) are a highly diverse family of enveloped positive-sense single-stranded RNA viruses.”
Coronavirus biology and replication: implications for SARS-CoV-2 https://www.nature.com/articles/s41579-020-00468-6 (2021)
“More than 700 recombinations were detected, with genes encoding major antigens frequently affected. Among these were 10 capsule-switching events, one of which accompanied a population shift as vaccine-escape serotype 19A isolates emerged in the USA after the introduction of the conjugate polysaccharide vaccine.”
Rapid Pneumococcal Evolution in Response to Clinical Interventions https://www.science.org/doi/abs/10.1126/science.1198545 (2011)
“Acellular vaccines against Bordetella pertussis were introduced in Australia in 1997. By 2000, these vaccines had replaced whole-cell vaccines. During 2008–2012, a large outbreak of pertussis occurred. During this period, 30% (96/320) of B. pertussis isolates did not express the vaccine antigen…”
“These findings suggest that B. pertussis not expressing [the vaccine antigen] arose independently multiple times since 2008…”
“This pattern is consistent with continuing evolution of B. pertussis in response to vaccine selection pressure.”
“…the combination of SNP typing, antigen gene typing, and prn [vaccine antigen] gene disruption mechanisms clearly demonstrates that isolates that do not express the prn gene from Australia and other countries do not belong to the same clone and that the recent almost simultaneous appearance and expansion of prn-negative isolates in several countries were independent events rather than global spread of a single clone.
The multiple origins of prn-negative isolates also point strongly to selective pressure on the bacterium. Therefore, it is conceivable that these prn-negative isolates are more likely to evade a vaccine-induced immune response.”
Rapid Increase in Pertactin-deficient Bordetella pertussisIsolates, Australia https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC3966384/ (2014)
“…significant changes in B. pertussis populations have been observed after the introduction of vaccinations, suggesting a role for pathogen adaptation in the persistence and resurgence of pertussis. These changes include antigenic divergence with vaccine strains and increased production of pertussis toxin.”
Pertussis resurgence: waning immunity and pathogen adaptation – two sides of the same coin https://pubmed.ncbi.nlm.nih.gov/23406868/ (2014)
Facebook post from Evergreen Health, a public hospital district in Washington state: https://www.facebook.com/127200785050/posts/10166194212020051/?d=n